This document discusses various risks associated with drugs used to treat ADHD. It addresses risks such as sudden death, hypertension, tachycardia, prolonged QT interval, psychiatric issues, seizures, growth effects, sleep problems, tics, liver toxicity, and more. For each risk, it provides information on frequency of association, evidence of causality, impact/severity, moderating factors, differences between drug effects, and considerations around modifying or managing the risks.
Nelamangala Call Girls: 🍓 7737669865 🍓 High Profile Model Escorts | Bangalore...
Templates Overview With Liver
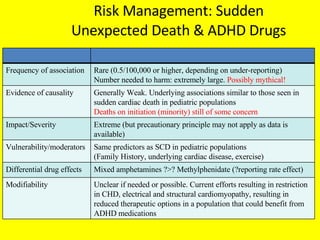
1. Risk Management: Sudden Unexpected Death & ADHD Drugs Frequency of association Rare (0.5/100,000 or higher, depending on under-reporting) Number needed to harm: extremely large. Possibly mythical! Evidence of causality Generally Weak. Underlying associations similar to those seen in sudden cardiac death in pediatric populations Deaths on initiation (minority) still of some concern Impact/Severity Extreme (but precautionary principle may not apply as data is available) Vulnerability/moderators Same predictors as SCD in pediatric populations (Family History, underlying cardiac disease, exercise) Differential drug effects Mixed amphetamines ?>? Methylphenidate (?reporting rate effect) Modifiability Unclear if needed or possible. Current efforts resulting in restriction in CHD, electrical and structural cardiomyopathy, resulting in reduced therapeutic options in a population that could benefit from ADHD medications
2. Risk Management: Hypertension & ADHD Drugs Frequency of association BP elevation common. 5-10% have hypertension Evidence of causality With Elevation: Strong, Might be unmasking essential hypertension as opposed to causing hypertension Impact/Severity Moderate to High due to long-term morbidity Vulnerability/moderators Effects of therapy untested within ADHD population Differential drug effects Need EMEA Data to determine Modifiability Effects of therapy untested within ADHD population, but effective agents are available in general population
3. Risk Management: Tachycardia & ADHD Drugs Frequency of association 0.9% (methylphenidate) Evidence of causality Generally Weak. Unclear documentation of improvement with withdrawal or recurrence with reinitiation Impact/Severity Mild to Moderate, symptoms may be intolerable Vulnerability/moderators ?Polypharmacy. Otherwise unknown. Differential drug effects unclear Modifiability Unclear. Assessment of ß-blockade response may be feasible. Other antiarrhythmics carry proarrhythmia risk. Potential for catheter ablation if needed to allow continuation.
4. Risk Management: QT & ADHD Drugs Frequency of association Suspicion, but no strong association Evidence of causality Weak, some evidence for HERG effect Impact/Severity Potentially high Vulnerability/moderators Co-prescription, ?undiagnosed underlying LQT condition Differential drug effects ?Atomoxetine > others? Modifiability Potential for ß-blocker therapy to modify risk (not QT interval)
5. Psychosis SUD Suicidility Anx/Dep Withdrawl Definition Frequency Rare NNTH>500 Causality mechanism O>E AE rate dose/response R e-challenge Weak Y N N N Impact Moderate Tolerable Transient self limiting Moderators/vulnerability e.g., Family history, mental retard, CV risk, Family history of psychosis? Differential Drug effects MTS>Modaf>DEX>ATX >MPH Modifiable caution with family history of psychosis Missing studies Caveat
6.
7. Height Weight BMI Growth disorder Definition Frequency Causality mechanism O>E AE rate dose/response rechallenge Dose for stimulants most studies support a dose response but some suggest only when dose > 1.5 mg/kg/day and when given continuously Impact Moderators/vulnerability e.g., Family history, mental retard, CV risk, Age Differential Drug effects Few data available, generally poor quality. 2/6 AMP > MPH, 4/6 AMP = MPH No studies Stim vs ATX Modifiable Missing studies Caveat
8. Height Weight Tics Sleep Irritability Definition Both results from objective and subjective studies must be considered. Increased sleep onset latency in some studies using methylphenidate Increased production of GH, one study Frequency unknown Causality mechanism O>E AE rate dose/response rechallenge Unknown Mechanism. Increase of wakefulness? Dose response ? Impact Unknown But may result in a (chronic?) reduction of total sleep time Moderators/vulnerabilit e.g., Family history, mental retard, CV risk, Unknown or not applicable Differential Drug effects Lack of head to head comparison studies Although one study with ATMX BID vs MPH TID by the company: ATMX>MPH for sleep onset latency Modifiable ? Or non applicable Missing studies Only few studies Conflicting results Lack of well designed trials Caveat Time of administration, pharmacokinetics of the drug, Cardio vascular and respiratory impact during sleep , not assessed Long term effects of MPH on sleep architecture and SWS per se, not documented
9. Social withdrawal in LD/ASD Irritability in LD/ASD Repetitive/stereotyped behaviour in in LD/ASD Definition Lack of interest in others; decreased responsiveness/orientation to others Increased negative response to minor/no provocation, elicited by parent/child questioning (variable threshold Frequency High baseline rates in ASD Definition dependent Severe ~2% High baseline rates in ASD Causality mechanism O>E AE rate dose/response rechallenge Weak 0/. Studies report increase in LD (MPH) 0/1 studies report increase in ASD (MPH) but non significant increase in % affected 0/1 study significantly improved in ASD (ATX) Weak, 1/1 reports increase n ASD at med. But not high dose (MPH) 0/3 report increase in LD (MPH) 0/1 increase in ASD (ATX) Weak 0/3 studies show increase, 1 shows sign decrease in LD (MPH) 0/1 shows increase in ASD (MPH) 0/1 study showing increase in ASD (ATX Impact Likely Moderate Likely Moderate Likely Moderate, Moderators/vulnerability e.g., Family history, mental retard, CV risk, None known None known None known Differential Drug effects Not known Not known Not known Modifiable Possible dose dependent Not known Possible dose dependent Missing studies No long-term studies Missing studies with adequate dosing in LD No ATX studies in LD No long-term studies Missing studies with adequate dosing in LD No ATX studies in LD No long-term studies Missing studies with adequate dosing in LD No ATX studies in LD Caveat Low power in studies to detect effect only mean scores evaluated so subgroup analyses All studies crossover Low power in studies to detect effect only mean scores evaluated so subgroup analyses All studies crossover Low power in studies to detect effect only mean scores evaluated so subgroup analyses All studies crossover
10.
11.
12.
13.
14. SUD in ADHD SUD by ADHD Med ADHD Med diversion Frequency Frequent (15% vs 5% of controls) see SUD & ADHD: ( no increase, could be a decrease ) Varying 5-35% Causality Weak , but high in comborbid CD or family load (ADHD+ SUD) No, (could be protective : early treatment, animal model) likeability? Impact Moderate to High low significant Moderator/ vulnerability Conduct Dis. ( hyperactivity) Age at start of Tx and at Follow up ( for putative protective effect) Age Enviroment ( access, motivation; ethnicity, income ?) Differential Drug effects N/A AMPH=MPH ATMX no long term data AMPH=MPH No ATMX IR > ER stim. Modifiable early med ?? ( before age 8 ) by continuing ADHD Tx ??? Stimulants vs Non-stim. ( formulation? )
15.
16.
17.
18. Mania Definition treatment-emergent mania, hypomania Frequency Rare ? ( RCTs : 0.19-0.25% of patients on active drugs, or ~ 1.5 per 100 person-years; Case series : ~6% ) Causality mechanism O>E AE rate dose/response rechallenge likely dopaminergic mechanism (?) ? ? ? Preclinical / animal data Methamphetamine and MPH mimic symptoms of mania in rats/mice Impact Moderate Tolerable if benefits substantial Transient (?) self limiting Moderators / vulnerability No risk factors identified in the majority of reports Differential drug effects occurred during double-blind treatment with every compound; complete absence of such events with placebo treatment Modifiable Predisposing: younger age? positive family history for mood disorders? Missing studies Sufficient duration of exposure to determine infrequent adverse events Caveat Much higher incidence in case studies than in RCTs! Some studies do not differentiate manic symptoms, “true” mania, irritability, psychosis; Information about resolution of symptoms often not provided